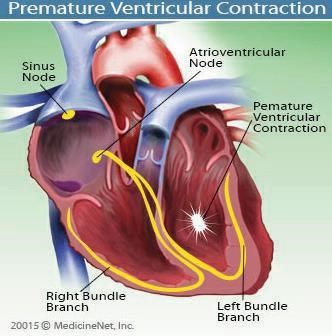
The heart has two upper chambers (atria) and two lower chambers (ventricles). In normal rhythm, the heartbeat begins in the sinoatrial (SA) node, which is the heart’s natural pacemaker in the right upper chamber. The SA node sends out an electrical signal that causes the atria to contract. This signal then moves throughout the heart’s electrical conduction system, later causing the ventricles to contract. With a PVC, however, the electrical signal starts earlier than it should and originates from a site in the bottom chambers of the heart.
The pattern is a normal beat followed by an extra beat (the PVC), then a slight pause (during which the electrical system of the heart resets, and the heart fills with more blood), and then a stronger-than-normal beat. People can be asymptomatic or may have symptoms related to the pause or the subsequent forceful beat after the PVC.
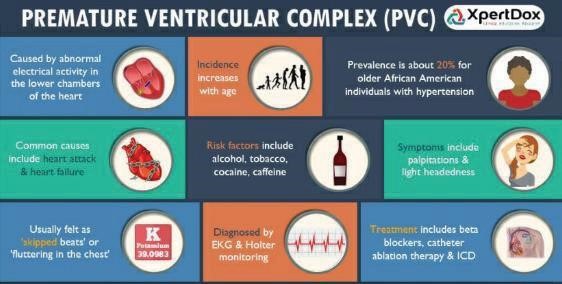
Many people with PVCs are asymptomatic and may not even know that they have them. Others may have symptoms that range from mild to severe, depending on the individual and the frequency of the PVCs.
The reasons for treating premature ventricular contractions are to relieve symptoms of palpitations, to treat conditions that cause premature ventricular contractions since many conditions that cause premature ventricular contractions are potentially life-threatening, and to prevent ventricular tachycardia and sudden death.